“High-Fiber Diet Might”, a translation
In this month’s JAMA Network Open we have an opinion piece [1] that struck a chord with me — a discordant, grating, and tuneless chord. I thought I’d share with you what I heard, when I read it, just to do my part in spreading the pain. Italics for the author’s word, bold for my translation, and footnotes for further commentary.
High-Fiber Diet Might Protect Against Range of Conditions
The popularity of low-carb diets, such as Atkins and keto, have helped give the macronutrient a bad name, and in part, it’s deserved.
Translation: We concede that carbohydrates are contributing to health problems, but we weren’t wrong. We never meant all carbohydrates were good, just the good ones!
“Have carbs got a bad reputation? Certainly…for a very understandable reason,” said Jim Mann, MB, ChB, PhD, a professor in human nutrition and medicine at the University of Otago in New Zealand. “They are highly refined, and, in many countries, sugar intake is high.”
But just as there are “bad” fats and “good” fats, there are also bad carbs and good carbs. “We showed very clearly in our work in diabetes that the benefits of carbs came from the good carbs, and the good carbs are not high in sugar,” Mann said. “They are high in fiber.”
Translation: In fact, we’ve shown that the benefit from carbs come from those carb foods that are low carb.
Mann, who spent years helping to hammer out the World Health Organization’s definition of fiber, recently coauthored a series of systematic reviews and meta-analyses that showed intake of fiber and whole grains—probably due to their high fiber content—but not foods with a low glycemic index was associated with significant reductions in mortality and chronic illnesses. (Breakfast cereals and other manufactured whole grain products are more highly processed today, so they provide less fiber and, likely, fewer health benefits, the authors noted.)
Translation: Mann spent years trying to help the WHO find a definition of fiber that would only include those fibers that had the properties they wanted to claim for it.(see image below from the cited paper [2] and further ironies). He recently coauthored a series of papers trying to retroactively support recommendations for high fibre intake.(Also, please don’t mistake our recommendation of whole grains to mean we’re recommending actual breakfast cereals or products that say “whole grains” on them).
Observational data suggested a 15% to 30% decrease in all-cause and cardiovascular-related mortality and incidence of coronary heart disease, stroke, type 2 diabetes, and colorectal cancer in people who consumed the most dietary fiber relative to those who consumed the least, the authors found. In addition, clinical trials showed that compared with low intake, high dietary fiber intake lowers body weight, systolic blood pressure, and total cholesterol. Given that the findings from prospective observational studies and clinical trials were complementary and that there was evidence of a striking dose response, the relationship between a high-fiber diet and lower disease risk could be causal, the authors concluded.
Translation: The meta-study (see quotes from it in the notes [3]) suggests that our recommendations might have had some basis, especially when we play the mind-game of expressing the weak-looking relative risks in absolute terms instead.
Although high-fiber intake is associated with lower weight, which in turn reduces the risk of diabetes, cardiovascular disease, and many cancers, dietary fiber appears to have benefits independent of its effect on weight, Mann said.
These findings and others suggest that virtually anyone who wants to lower their risk of a variety of ailments—including cardiovascular disease and multiple types of cancer, such as ovarian, pancreatic, and liver as well as colorectal—should consume more, not fewer, carbs, as long as they’re good carbs, ie, fiber-rich whole grains, legumes, fruits, and vegetables.
Translation: When we adjust for weight loss associated with these lower-carb carbs, much of the already small correlation goes away. Therefore it makes sense that this recommendation to eat higher fibre should be applied to anyone who doesn’t want to die a horrible death.
However, in westernized countries, few people consume anywhere near the recommended amounts of dietary fiber. In the United States, the average dietary fiber intake by adult men and women is 18 g and 15 g, respectively, based on the 2013-2014 National Health and Nutrition Examination Survey (NHANES) data. And yet, the 2015-2020 Dietary Guidelines for Americans recommends a daily minimum intake of 33.6 g per day for men and 28 g for women 19 to 30 years of age, and only slightly decreasing amounts as people get older.
Translation: No one is paying attention to our guidelines. Even though our results are weak and there has been no causal link established, we recommend a fibre intake with a precision to the tenth of a gram to help convey our confidence.
And what about people who swear by a low-carb diet and, as a result, consume relatively little dietary fiber?
“In the short-term, if a person has a very high body mass index, almost anything that would cause weight loss would be beneficial,” said Edward Giovannucci, MD, ScD, a professor of nutrition and epidemiology at the Harvard T.H. Chan School of Public Health. “In the long-term, it’s a different story,” Giovannucci said, noting a lack of long-term studies of low-carb diets.
Translation: Please don’t confuse your actual results with the power of our statistical model. We don’t have enough data on what you’re doing to show if the benefit you’re experiencing in practice works in theory. Nor have we bothered to learn enough about it to realise it can be implemented with or without high fibre.
Figuring Out Fiber
An early theory for why dietary fiber was inversely related to colon cancer risk was mechanical: Fiber quickens the transit time of stool by bulking it up. There might be some truth to that explanation for why fiber intake and colon cancer risk are inversely related, said Giovannucci, who served on the American Institute of Cancer Research panel that produced a recent report on the relationship between diet, nutrition, and physical activity and colon cancer. “Certainly, you would think fiber would be more relevant to the diseases of the colon,” he said.
Translation: We’ve had this intuitive theory that fibre might be protective of colon cancer for a long time, since it goes through the colon when you eat it.
Indeed, “the lack of fiber is particularly pertinent to the remarkably high incidence rates of colon cancer in westernized societies,” Stephen O’Keefe, MBBS, MD, FRCP, wrote in a recent article. “In stark contrast, colon cancer is rarely seen in rural African communities consuming their traditional high-fiber (≈50 g/d), low-meat, and low-fat diets.”
Translation: Westerners have higher rates of colon cancer than non-westerners, including those that eat higher fibre diets low in meat and fat,(and those that eat lower fibre diets high in meat and fat, but we don’t talk about that).
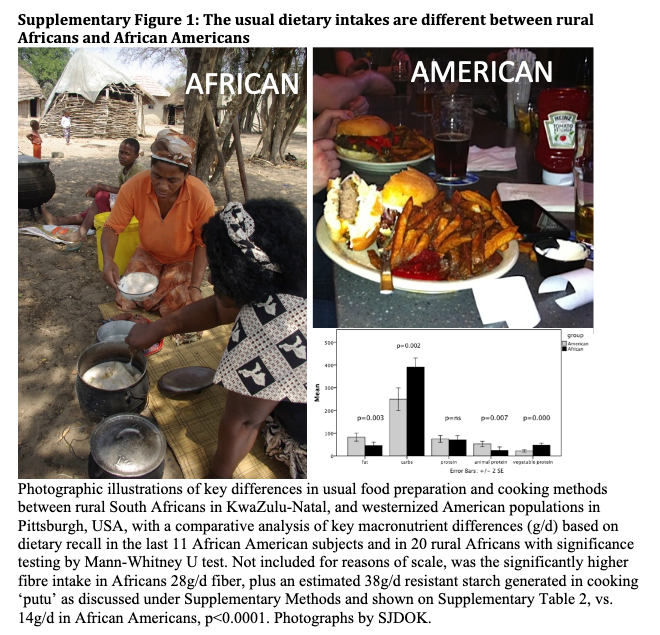
In 2015, O’Keefe coauthored a widely cited study in which 20 African Americans and 20 rural Africans swapped their regular diets for 2 weeks. The researchers prepared high-fiber (50 g/d), low-fat African-style meals for the African Americans and high-fat, low-fiber meals for the rural Africans.
The brief diet swap was long enough for the scientists to observe reciprocal changes in participants’ gut microbiota and metabolome, which were associated with changes in mucosal biomarkers of cancer risk. The authors emphasized that changes in animal protein or digestible carbohydrate intake associated with changes in dietary fiber consumption could also have contributed to the observed mucosal alterations. They concluded that their results raise the hope that increasing fiber consumption, along with moderating fat intake, could reduce African Americans’ disproportionately high incidence of colon cancer.
Translation: Since we can’t do a trial for long enough to to measure what we care about, we are trying to find other support for the idea that fibre is protective of colon cancer. For example we can compare intestinal bacterial effects of traditional foods from rural South Africa, to a diet of french fries and burgers with ketchup, and see if any of the microbiome responses correspond to another body of epidemiological associations that might be more predictive than the ones we already have [4]. As you can see in the photo, lack of fibre is the clear difference in this study.

Dietary fiber appears to be protective even after a diagnosis of colorectal cancer, Giovannucci and his coauthors suggested in a recent JAMA Oncology article. Using data from the Nurses’ Health Study and the Health Professionals Follow-up Study, they found that higher fiber intake after a diagnosis of nonmetastatic colorectal cancer was associated with a lower risk of death from that disease and all causes.
“Higher intake of fiber, especially cereal fiber, has been linked to improved insulin sensitivity, lipid profile, endothelial function, and reduced inflammation,” and evidence is just beginning to suggest that hyperinsulinemia and markers of insulin resistance and inflammation predict worse survival in patients with colorectal cancer, Giovannucci and his coauthors note.
Translation: Although we don’t have trials supporting high fibre diets in those diagnosed with colon cancer, we have some more weak associations that suggest it would [5]. The associations for fruit and vegetable fibres are particularly weak, even by our standards, so we won’t mention them specifically. This association might in turn be just a reflection of the association between higher fibre intake and metabolic syndrome symptoms, which is independently predictive, but instead of suggesting that we take measures to reduce metabolic syndrome, we’ll continue to recommend the fibre itself.
In other words, the explanation for why a high-fiber diet appears to be protective goes far beyond speeding stool’s conveyance through the colon. And, it turns out, fiber’s health benefits extend beyond the colon as well.
Translation: So, never mind about the initial explanation we tried to use to justify our hypothesis. Let’s move on to something even less intuitive.
For example, a recent study involving participants in the Prostate, Lung, Colorectal, and Ovarian (PLCO) cancer screening trial found an inverse association between dietary fiber intake and head and neck cancer, particularly oral cavity and pharyngeal tumors.
“We have found the inverse association between dietary fiber and head and neck cancer risk not only among smokers and drinkers but also among never smokers and never drinkers,” said coauthor Daisuke Kawakita, MD, PhD, of the Department of Otorhinolaryngology, Head and Neck Surgery, Nagoya City University Graduate School of Medical Sciences in Japan.
The late British surgeon Denis Burkitt, FRS,—aka the “Fiber Man”—popularized the notion a half-century ago that dietary fiber protected against a host of diseases, but not until recently have scientists begun to explain “the whole biochemistry of how fiber can have distal effects all around the body,” said O’Keefe, a University of Pittsburgh gastroenterologist.
Translation: In order to try to confirm our hypothesis about the association between fibre intake and cancer, we’ll divide and conquer. By retroactively dividing the set of diseases into different classes, we can manipulate the size of the associations by choosing which sets to report on. We can revisit the same data set over and over again with different hypotheses until one of them statistically pans out. This is often called “data dredging” or “p-hacking”, but those words have unpleasant connotations.
O’Keefe and others posit that fiber’s effect on gut microbiota may explain its health benefits for the colon and beyond. “The metabolites of fiber, particularly butyrate, can prevent cancer in any part of the body,” he said.
Butyrate, a short chain fatty acid that serves as a fuel source for the cells that line the colon, facilitates apoptosis of colonic cancer cells and reduces gut inflammation, note the authors of a 2017 review article about butyrate in the colon and peripheral tissues. As the authors write, research has shown that increased fiber consumption or oral butyrate supplementation has been shown to decrease adiposity and improve insulin sensitivity.
Translation: The most promising current potential mechanism to lend plausibility to the fibre hypothesis is that fibre is broken down into butyrate by gut bacteria. Butyrate , (which can come from other sources besides dietary fibre), has been shown to have benefit in the colon, (probably because it breaks down into the ketone body beta-hydroxybutyrate [6]). As per the paper we cite, [7] butyrate from fibre that makes it into the bloodstream is captured by the liver and metabolised. So butyrate doesn’t actually reach peripheral tissues. However, if we supplement butyrate so that it does reach them, it can improve insulin resistance. Glossing over these details, we can then make it sound like butyrate from dietary fibre has benefits across the body.
But are the apparent health benefits from consuming foods naturally high in fiber due to fiber itself or to other nutrients that accompany it?
The correct answer is both, O’Keefe said. Dietary fiber is a marker for other nutrients in naturally fiber-rich foods, particularly phytochemicals, and at the same time it is also a biomolecule, he said. Plus, O’Keefe said, “People who eat fiber-rich foods are health conscious as well. Their lifestyle is better.”
Translation: Can’t all this association be explained by the other things people who eat fibre eat and do? Yes. It could totally be from the health-conscious nature of people who eat fibre, but we really think it’s about the plants, and we’re doing our best to come up with theories about how that could be true. For example, we’re branching out our search for a benefit from plants into other non-nutritive chemicals they contain. Fibre is still a biomolecule, it’s got to have a positive effect.
Fiber in a Pill?
These days, it’s possible to find high-fiber brownies and high-fiber ice cream in many supermarkets. Of course, the only reason they’re high in fiber is because synthetic or isolated fiber was added to them.
Besides flour or milk, their labels list such ingredients as soluble corn fiber—“produced from corn through enzymatic hydrolysis of corn starch,” according to an industry website—or sugarcane fiber, also used to make plates and bowls.
“They do seem to be able to lower cholesterol a bit, but we do not know whether those synthetic or extracted fibers have the same long-term benefits,” said Mann, who, to illustrate this point in lectures, uses a slide of a high-fiber English muffin sold in the United States. A check of the ingredients of high-fiber English muffins is likely to reveal that their fiber comes from an additive such as cellulose, not whole wheat flour.
As Giovannucci said, “In most of the observational studies that are the basis of most of the data and recommendations, what we really studied are the whole foods.”
Translation: It’s really important to understand that the proposed benefit we’re attributing to fibre isn’t attributable to fibre, but to foods that contain fibre. It’s not really about the fibre. Fibre is used for making plates! So just eat whole foods with lots of fibre. Ok?
Still, when the US Food and Drug Administration (FDA) in 2016 finalized its Nutrition Facts and Supplement Facts Label, with the agency’s first-ever definition for dietary fiber, it included 7 isolated or synthetic nondigestible carbohydrates, such as cellulose and guar gum, as well as “intrinsic and intact” fibers in plants.
Based on small, short-term clinical trials, the agency said, the isolated or synthetic carbohydrates had “physiological effects that are beneficial to human health,” such as lowering blood glucose or cholesterol or increasing the frequency of bowel movements.
Translation: Well maybe it is about the fibre. Anyway, how else could you lower your blood sugar? As a bonus you get lower cholesterol and you get to poop more. These have both been equally shown to improve health, as I’m sure we don’t have to explain.
In June, the FDA released a scientific review of 8 more added nondigestible carbohydrates it plans to include in its definition of dietary fiber. However, none of the research cited by the FDA looked at the long-term impact, namely disease risk, of the 15 added nondigestible carbohydrates. In late March, the FDA announced plans to propose that manufacturers be allowed to identify a 16th nondigestible carbohydrate as dietary fiber on food labels.
Added fiber is better than no fiber, O’Keefe said, but “we’re designed to eat a balanced diet, and a balanced diet comes from what’s available naturally.”
Translation: So, we know fibre is good for you based on weak long-term associations that in all likelihood have to do with other components of the diet or behaviour of the subjects. That doesn’t change our conviction that it is still better to get fibre from other sources than not at all, especially since now we can use these food additives to put health claims on labels. When you get your fibre this way and are still unhealthy, we can remind you that we never said that isolated fibre had health benefits.
Feasting on Fiber
Mann said he typically consumes at least 40 g of fiber a day, which might seem daunting to most people in westernized countries. “It does require a bit more preparation,” Mann noted. “If people are not well off, it’s cheaper to go and buy a Big Mac.”
Indeed, the NHANES data found that higher income was associated with higher fiber intake, although there are other explanations for that relationship besides the cost of high-fiber foods.
Translation: Basically, the reason we’re finding this association is that rich people tend to be healthier and they also eat more fibre whereas poor people tend to be unhealthier and they also eat more Big Macs.
Increasing dietary fiber intake doesn’t have to be expensive. Mann, O’Keefe, and Giovannucci all pointed to legumes, which include beans, chickpeas, and lentils. A good source of protein as well as fiber, legumes are “a particularly underutilized food,” Giovannucci said.
Translation: You, too, can have the health of the wealthy if you’d just spend more time cooking these evidently undesirable and unappealing foods. Poor people have more time than rich people. It’s not like time is money.
Experts emphasize the need for public health messages about the value of consuming more dietary fiber and how to do it.
“We need a population push, just a bit like the lung cancer story,” O’Keefe said, referring to the worldwide decline in smoking rates. “The information’s got to get out to the population to understand the clear significance and strong relationship between fiber intake and various kinds of cancer and westernized diseases.”
Translation: If we get the narrative right, we can make people believe that hazard ratios of 1.2 or 1.3 are as meaningful as hazard ratios of 20. We just have to push people more.
That’s the state of the art, folks.
References and Notes
[1] Medical News & Perspectives, April 17, 2019, High-Fiber Diet Might Protect Against Range of Conditions, Rita Rubin, MA, JAMA. 2019;321(17):1653-1655. doi:10.1001/jama.2019.2539
[2] Cummings, Jh, Ji Mann, C Nishida, and Hh Vorster. “Dietary Fibre: An Agreed Definition.”The Lancet 373, no. 9661 (January 2009): 365–66.
In this paper Mann and his colleagues also make clear that although even the epidemiological evidence fails to show benefit, whatever substances they can support as beneficial with experiments using extracts from food should not get the label when they are sold as extractions, but only when sold to match the epidemiological data.
“[B]ecause long-term epidemiological evidence of health benefit is lacking, the definition requires generally accepted scientific evidence to be presented to competent authorities before such polymers can be labelled as fibre…
“Calling [oligosaccharides] fibre is potentially misleading for consumers. For example, bottled water with some of these substances added could be sold as a source of fibre. Consumers might then be tempted to obtain the recommended fibre intake from such products rather than from fruit, vegetables, and wholegrain cereals.”
In the end it gets the desired label, though.

[3] Reynolds, Andrew, Jim Mann, John Cummings, Nicola Winter, Evelyn Mete, and Lisa Te Morenga. “Carbohydrate Quality and Human Health: A Series of Systematic Reviews and Meta-Analyses.”The Lancet 393, no. 10170 (February 2019): 434–45.
“Quantitative recommendations relating to dietary fibre do not have a strong evidence base.”
“Findings from prospective studies and clinical trials associated with relatively high intakes of dietary fibre and whole grains were complementary, and striking dose-response evidence indicates that the relationships to several non-communicable diseases could be causal. Implementation of recommendations to increase dietary fibre intake and to replace refined grains with whole grains is expected to benefit human health.”
The “striking” observed correlations combined to an all-cause mortality relative risk RR 0·85 (0·79 to 0·91), which the authors consider to be “moderate” evidence. I consider this rather generous.
[4] O’Keefe, Stephen J. D., Jia V. Li, Leo Lahti, Junhai Ou, Franck Carbonero, Khaled Mohammed, Joram M. Posma, et al. “Fat, Fibre and Cancer Risk in African Americans and Rural Africans.”. Nature Communications 6 (April 28, 2015): 6342.
[5] Song, Mingyang, Kana Wu, Jeffrey A. Meyerhardt, Shuji Ogino, Molin Wang, Charles S. Fuchs, Edward L. Giovannucci, and Andrew T. Chan. “Fiber Intake and Survival After Colorectal Cancer Diagnosis.”. JAMA Oncology 4, no. 1 (January 1, 2018): 71.
[6] Does a ketogenic diet confer the benefits of butyrate without the fibre?
[7] McNabney, Sean M., and Tara M. Henagan. “Short Chain Fatty Acids in the Colon and Peripheral Tissues: A Focus on Butyrate, Colon Cancer, Obesity and Insulin Resistance.”. Nutrients 9, no. 12 (December 2017): 1348.